Clinical Evidence: Fat Distribution’s Impact on Cardiometabolic Disease
Protection Against Cardiovascular Disease
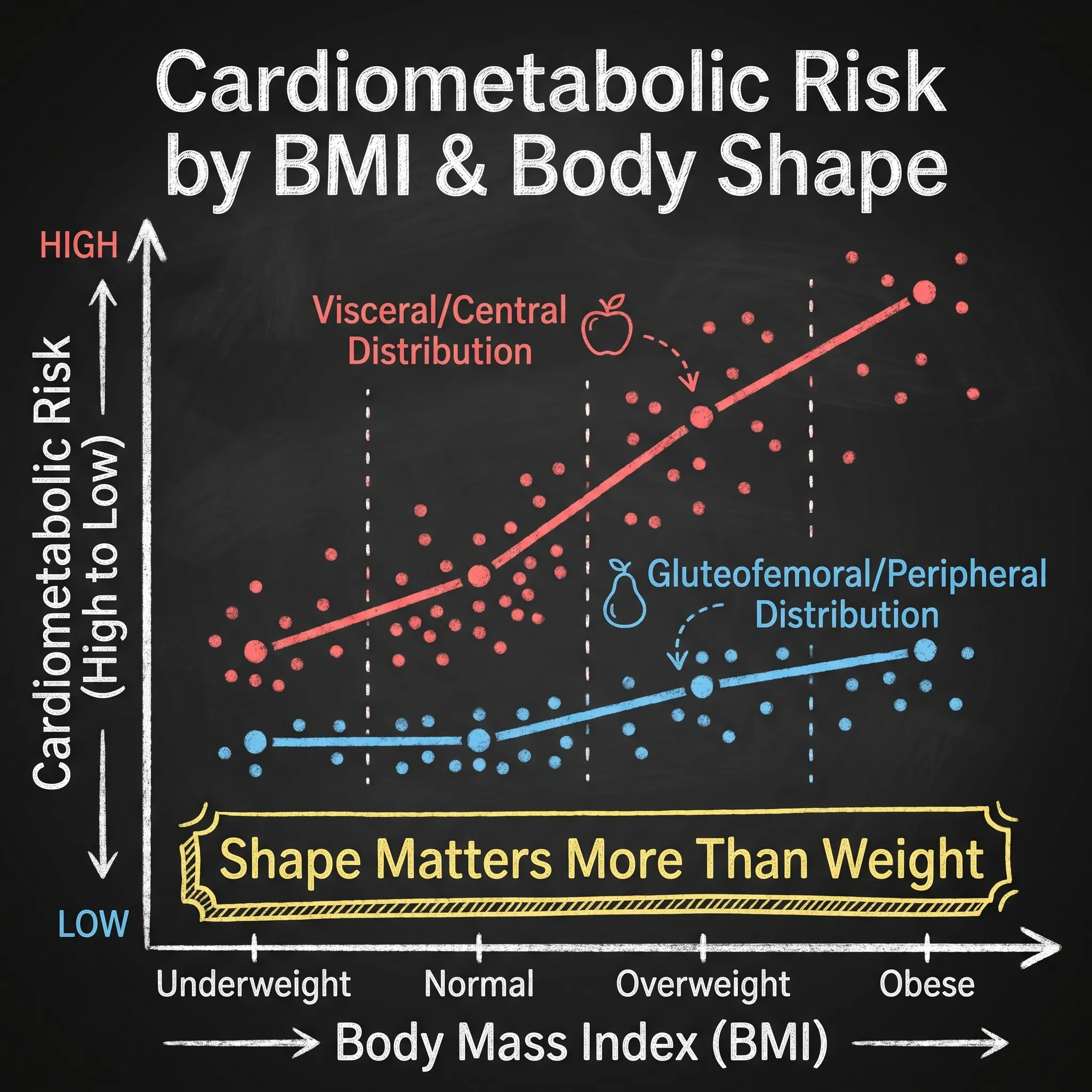
Recent clinical evidence highlights that fat distribution and cardiometabolic health are inextricably linked, suggesting that where the body stores fat is a more critical predictor of disease than total body weight or BMI.
Multiple prospective studies confirm that gluteofemoral fat distribution provides independent protection against cardiovascular disease.
Large epidemiological studies demonstrate that peripheral body fat distribution clearly dissociates fat mass from metabolic disease risk.
Recent Mendelian randomization studies, which imply causation using genetic variants, show that genetically predicted higher gluteofemoral fat volume is associated with:
- Lower LDL cholesterol
- Higher HDL cholesterol
- Lower triglycerides
- Reduced systolic and diastolic blood pressure
- Decreased type 2 diabetes risk
Stroke and Cerebrovascular Protection
Emerging evidence extends the protective effects of gluteofemoral fat beyond metabolic syndrome to neurological outcomes. Genetic predisposition to higher gluteofemoral fat volume is associated with:
- Lower ischemic stroke risk
- Lower large artery stroke risk
- Lower small vessel stroke risk
- Reduced carotid intima-media thickness (a marker of atherosclerosis)
Notably, this protective effect operates independently of body mass index, suggesting that fat distribution, itself, drives the cardiovascular benefits.
Metabolic Syndrome Components
In the Jackson Heart Study, while both abdominal visceral and subcutaneous fat were positively correlated with metabolic dysfunction, visceral adipose tissue deposition was most strongly associated with hypertension, type 2 diabetes, and metabolic syndrome risk.
In contrast, gluteofemoral subcutaneous fat accumulation was not associated with metabolic syndrome risk, and in many studies showed protective associations.
The Visceral Fat Problem: A Cautionary Tale
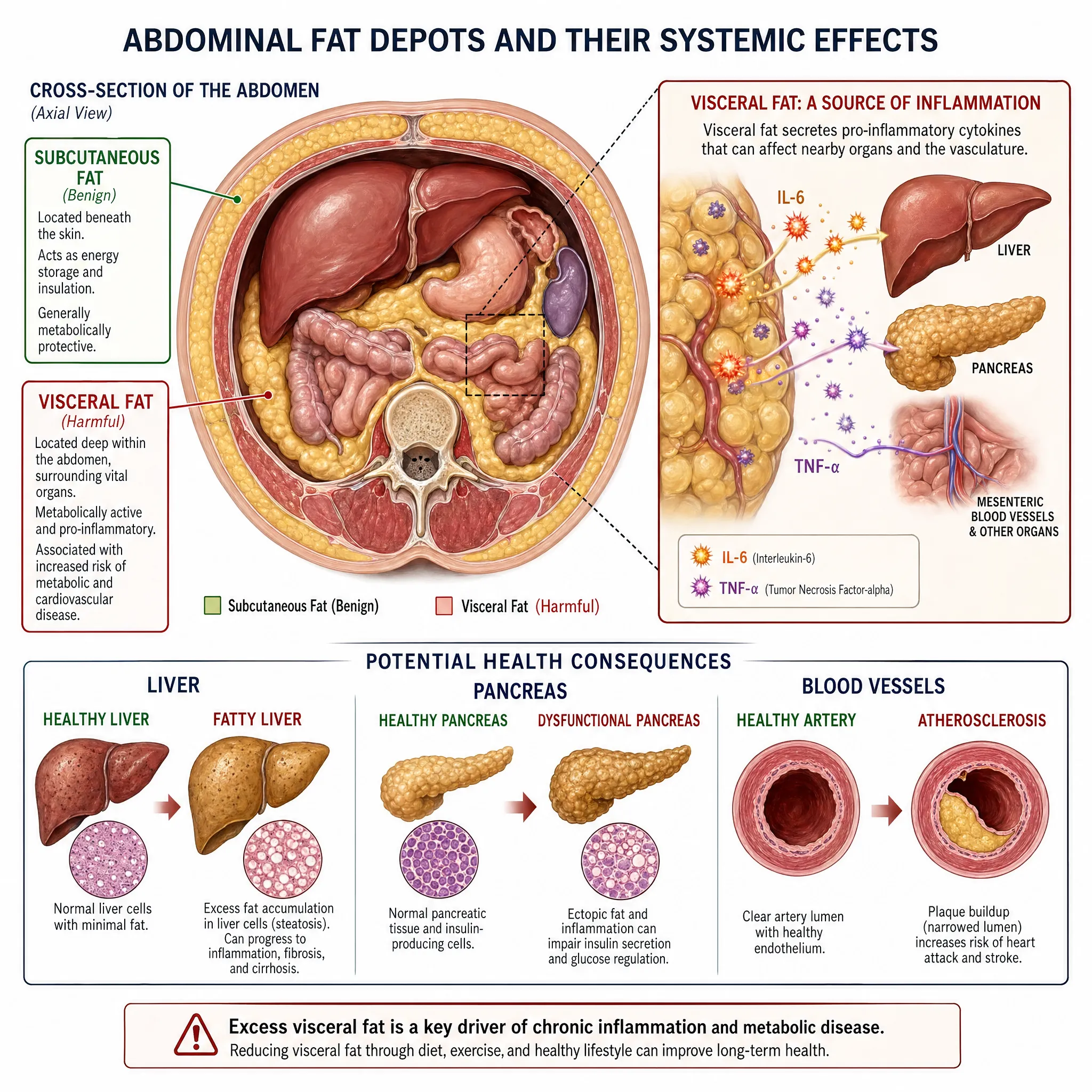
While peripheral fat appears metabolically benign, visceral fat tells a very different story. Visceral adipose tissue actively secretes elevated levels of pro-inflammatory cytokines, including IL-6 and TNF-α, while reducing protective adipokines like adiponectin. This pro-inflammatory environment contributes to:
- Insulin resistance and glucose dysregulation
- Oxidative stress and endothelial dysfunction
- Fatty liver disease
- Atherosclerosis acceleration
- Dyslipidemia and hypertension
Alarmingly, visceral fat shows strong associations with dysregulated glucose homeostasis even in non-obese individuals, highlighting its particularly toxic metabolic effects.
Practical Health Implications for Clients
1. Preservation of Peripheral Fat Capacity
An elegant clinical observation revealed that when women had thigh fat surgically removed via liposuction, the fat was subsequently re-accumulated preferentially in the abdominal area. This demonstrates that peripheral fat depots serve as the body’s preferred “safe storage facility”, when that capacity is compromised, harmful central fat accumulation accelerates.
Clinical implication: Rather than aggressive fat reduction in all regions, effective wellness strategies should focus on preventing visceral fat accumulation while maintaining healthy subcutaneous peripheral depots.
2. Understanding Sex-Specific Adipocyte Biology
Women demonstrate distinct adipocyte characteristics that contribute to their metabolic advantage:
- Gluteofemoral adipocytes are larger in women than in men, increasing storage capacity
- Abdominal adipocytes are comparable between sexes, but women start with more adipocytes even at lean body weight
- Visceral adipocytes are smaller in women, limiting harmful visceral expansion
When women gain weight, subcutaneous expansion occurs primarily through hyperplasia (new adipocyte formation), while men experience hypertrophy (enlargement of existing adipocytes). This fundamental difference in expansion strategy may explain why women can accommodate larger fat masses without metabolic deterioration.
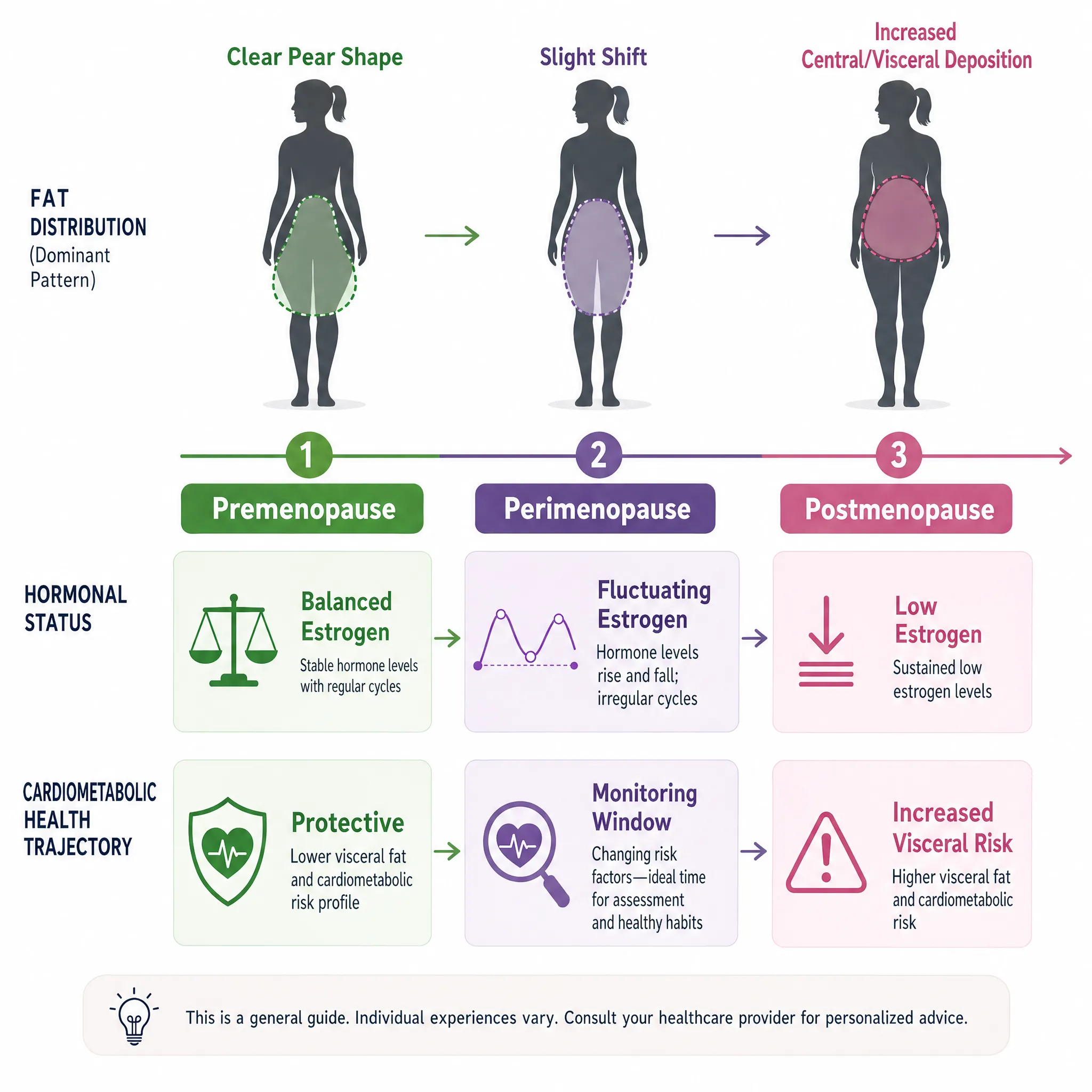
3. Hormonal Windows and Menopause Transitions
For women, especially those approaching perimenopause and menopause, hormone-aware health strategies become increasingly critical. The dramatic shift in fat distribution accompanying menopause isn’t merely cosmetic; it reflects fundamental changes in metabolic health trajectory.
Clinical implication: Menopause represents a critical intervention window where targeted strategies to preserve metabolic health and prevent visceral fat accumulation become especially important.
4. Moving Beyond BMI as a Health Metric
The research is unequivocal: BMI is an inadequate proxy for metabolic health or disease risk. Multiple studies demonstrate that hip-to-waist ratio, waist circumference, or imaging-based measures of fat distribution are far more accurate predictors of cardiometabolic disease than body mass index.
Clinical implication: Clients shouldn’t be alarmed by BMI readings if their fat is distributed peripherally. Conversely, lean clients with central adiposity warrant careful metabolic assessment and intervention.
5. Recognize the Complex Biology
Sex differences in adipose tissue function arise from a sophisticated interplay of:
- Genetic factors (explaining ~1% of variation)
- Epigenetic programming by hormones and lifestyle
- Cell-autonomous adipocyte properties related to sex chromosomes
- Depot-specific microenvironments that differ in vascular, neural, and immune characteristics
- Developmental factors including critical windows of hormonal imprinting
This complexity means that one-size-fits-all approaches to weight management are inherently flawed. Personalized strategies that account for individual genetic predisposition, current life stage, and existing fat distribution patterns are essential.
The Bottom Line: Body Shape as a Window into Metabolic Destiny
The research is increasingly clear: the biology of body shape profoundly influences metabolic health and disease risk. The “pear-shaped” distribution associated with women’s typical fat storage pattern isn’t simply an aesthetic difference, it reflects deep biological advantages in how the body handles energy storage, regulates inflammation, and maintains insulin sensitivity.
Rather than chasing arbitrary weight numbers or pursuing uniform thinness, a more scientifically grounded approach to wellness involves:
- Understanding individual fat distribution patterns through waist circumference, hip circumference, and ideally imaging assessment
- Supporting metabolic health through evidence-based interventions that preserve peripheral fat capacity while reducing visceral accumulation
- Recognizing life-stage transitions (particularly menopause) as critical intervention windows
- Honoring genetic and epigenetic complexity through personalized rather than standardized approaches
- Appreciating that healthy bodies come in different shapes for compelling biological reasons
The future of personalized wellness at lies in honoring this complexity and helping clients understand that their body’s unique shape may be exactly what they need for optimal metabolic health.
By moving beyond reductive metrics like BMI toward a more nuanced understanding of fat distribution and metabolic physiology, we can help clients make informed decisions that align with genuine health, not arbitrary aesthetic standards.
Further reading
- Gluteofemoral body fat as a determinant of metabolic health
- Subcutaneous and visceral adipose tissue: structural and functional differences
- Trunk fat and leg fat have independent and opposite associations with fasting and postload glucose levels: the Hoorn study
Disclaimer:
This information is for educational purposes only and does not constitute professional medical advice. Always consult a healthcare professional before incorporating any new therapy into your practice.
Do you want to see all the updates?
👉 Follow us on Instagram and Facebook and never miss a thing!


